Can Glaucoma Be Detected During Pregnancy?
- By Centre For Sight
- 7 minutes
|
Key Takeaways
|
If you are pregnant and concerned about eye pressure, it is natural to wonder whether glaucoma can be safely diagnosed and managed.
Pregnancy creates a unique challenge: while eye pressure often decreases, glaucoma may still worsen especially if medications are reduced.
This guide explains:
-
Whether glaucoma can be detected during pregnancy
-
Which tests are safe
-
How pregnancy affects eye pressure
-
How treatment is planned to protect both mother and baby
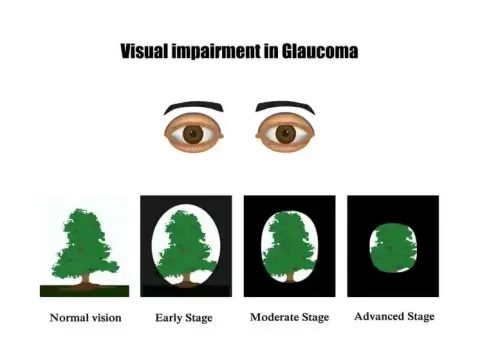
What Is Glaucoma and Why Is Pregnancy Tricky?
Glaucoma is a condition that damages the optic nerve, often associated with increased intraocular pressure. It is known as the ?silent thief of sight? because early stages usually have no symptoms.
Pregnancy complicates glaucoma care because:
-
IOP tends to decrease in later trimesters
-
Corneal thickness increases
-
Hormonal changes alter eye physiology
These changes can mask disease progression or affect measurement accuracy.
Can Glaucoma Be Detected During Pregnancy?
Yes. Glaucoma can be detected using the same core diagnostic tools used outside pregnancy.
However, interpretation is more nuanced. Doctors rely on a combination of findings rather than a single IOP reading.?
What glaucoma tests are used and why?
- Eye pressure (tonometry) is still important, but readings may be lower later in pregnancy. Meta-analysis data shows IOP drops significantly in the 2nd trimester (about ?1.53 mmHg) and 3rd trimester (about ?2.91 mmHg) versus non-pregnant measurements.
- Optic nerve exam checks for nerve cupping and change over time.
- OCT optic nerve imaging helps track structural change (useful when pressure is ?behaving? but the nerve isn't).
- Visual field tests show functional vision loss patterns; some studies note field results can fluctuate during pregnancy, so repeatability matters.
How Pregnancy Affects Glaucoma And Eye Pressure?
Many women experience a natural IOP decrease as pregnancy progresses. A review of ocular changes in pregnancy and a meta-analysis both support this general pattern, especially in the second half of pregnancy.?
Two key physiologic changes explain it clearly:
- Lower IOP in later trimesters shown consistently across studies.?
- Thicker cornea in pregnancy: AAO notes corneal thickness increases in the 2nd and 3rd trimesters due to water retention, which can influence measurements and temporary refraction changes.
Important reality check for women who already have glaucoma
Even though IOP decreases, glaucoma doesn't always ?settle down.? The Glaucoma Research Foundation cites a study where up to 60% of pregnant women with glaucoma had worsening visual fields and/or increased eye pressure during pregnancy, which is why close monitoring matters.?
A classic follow-up study (small sample, but useful) tracked 15 pregnant women with glaucoma and found:?
- 57.1% of eyes: IOP stable and no visual field progression
- 17.9% of eyes: Visual field progression with stable or increased IOP
- 17.9% of eyes: Stable fields despite increasing IOP
Important Note: Pregnancy responses vary, so your plan must be personal.?
Treatment Of Glaucoma During Pregnancy
This is the hardest part for most families: you need to protect the optic nerve, but you also want the lowest possible medicine exposure for the baby.
A major review notes that no topical glaucoma medication has strong human evidence proving safety, and most safety data comes from case reports or animal studies.?
|
Drop class |
Common examples |
Pregnancy notes |
Breastfeeding notes |
|
Alpha-2 agonist |
Brimonidine |
Discussed as a ?safer? option earlier, but data is limited |
Avoid (risk of CNS depression in newborn) |
|
Beta-blocker |
Timolol |
Longest track record used; still used cautiously |
Considered compatible by pediatric guidance in some reviews (dose-minimize) |
|
Carbonic anhydrase inhibitor |
Dorzolamide/Brinzolamide |
Used selectively when needed |
Considered acceptable in breastfeeding in some guidance (dose-minimize) |
|
Prostaglandin analog |
Latanoprost/Travoprost |
Avoided when possible due to theoretical concerns in pregnancy |
Case-by-case; discuss with doctor |
Note: This is general information. Final decisions depend on your trimester, glaucoma severity, and obstetric plan and must be decided by your doctor.
How To Reduce Medicine Exposure?
This is one of the most useful step for pregnant patients using drops:
Nasolacrimal occlusion (NLO) / eyelid closure
Closing the eyelids and pressing the inner corner of the eye (near the nose) reduces drainage into the tear duct.?A clinical reference reported that NLO or eyelid closure for 5 minutes reduced systemic absorption by over 60%.?
This is the kind of detail that makes glaucoma care in pregnancy safer without changing the actual treatment plan.?
Steps:
- Instill the eye drop
- Close the eye gently
- Press the inner corner of the eye (near the nose)
- Hold for 2?5 minutes
- Blot excess fluid
This can reduce systemic absorption by over 60%, improving safety without altering treatment.
Non-Drop Options That Can Reduce Medication Need
When doctors want to reduce fetal exposure, they look for options that lower IOP without daily drugs.
Laser trabeculoplasty (SLT/ALT)
Laser trabeculoplasty is widely discussed as a useful option for women planning pregnancy or during pregnancy because it can reduce or eliminate the need for drops in some cases.?
One recent clinical discussion reports SLT is effective in about 75% of patients, lowering pressure ?by a few points? (results vary by glaucoma type and baseline pressure).?
Surgery
Surgery is avoided during pregnancy if possible, but it can be considered if glaucoma is progressing despite maximum safe therapy. Added considerations in pregnant patients include anesthesia risk and the need for post-op medications.?
A Monitoring Plan By Trimester
This is the ?how doctors think? part, explained simply.
First trimester
This is the most sensitive phase for fetal development (organ formation), so many reviews recommend minimizing medications when safe and monitoring closely.?
Second and third trimester
IOP decreases, but it can still rise in glaucoma patients, so pressure checks and functional/structural monitoring remain important.?
Postpartum and breastfeeding
Pressure trends can shift again after delivery. One report notes pregnancy-related IOP decrease may last up to 2 months postpartum, so follow-up doesn't stop after childbirth.?
When To See An Eye Doctor Urgently?
Get urgent care if you have:
- Sudden eye pain with headache/nausea
- Sudden blur or halos with a ?hard? eye feeling
- Rapidly worsening vision or a new field defect feeling
- Severe redness with light sensitivity after starting/stopping drops
Conclusion
Glaucoma during pregnancy can be managed safely, but it needs a plan that balances optic nerve protection with fetal safety.?Pregnancy lowers measured eye pressure, yet studies show glaucoma can still worsen in a significant minority, which is why regular monitoring of pressure, optic nerve, and visual fields matters.?
The safest next step is coordinating your ophthalmologist and obstetrician early, ideally before conception or as soon as pregnancy is confirmed.?
FAQs
Can glaucoma be detected during pregnancy?
Yes, glaucoma can be detected during pregnancy and is detected with the same tests (IOP, optic nerve exam, OCT, visual fields), but doctors interpret results carefully because pregnancy can lower IOP and change corneal thickness.?
Does pregnancy lower eye pressure?
Yes, pregnancy can lower eye pressure but not always, meta-analyses show a significant average drop in the 2nd and 3rd trimesters, yet glaucoma patients can still have stable, rising, or fluctuating pressures depending on their disease and treatment changes.?
Are glaucoma eye drops safe during pregnancy?
Safety evidence in humans is limited for all drops, so doctors use the lowest effective dose and adjust by trimester; techniques like nasolacrimal occlusion helps reduce systemic absorption.?
What is the safest way to reduce glaucoma drop side effects while pregnant?
The safest way to reduce glaucoma drop side effects while pregnant is nasolacrimal occlusion or eyelid closure after instilling drops, which can reduce systemic absorption by over 60%.?
Can laser treatment replace glaucoma drops during pregnancy?
Yes, selective laser trabeculoplasty is discussed as a pregnancy-friendly option because it can reduce medication need and has no direct drug exposure to the fetus, though results depend on glaucoma type and baseline pressure.?


Could not find what you are looking for?



